All The Many Therapies in Dyslexia
There are many therapies that have been reported helpful in dyslexia. To date, each therapeutic endeavor has been often poorly understood and thus incompletely explained. And the absence of a theory that can bring all the helpful therapies under a common "umbrella" together has thus far resulted in a fragmented therapeutic approach. To make matters worse, since the effectiveness of most of these varied therapies tends to refute the thinking-brain processing theories of dyslexia, conflict was created rather than resulting in unbiased meaningful/comprehensive understanding.
Accordingly, the aim of this article is to provide readers with a simple unifying albeit highly summarized explanation as to how these varied therapies work. And as you will see, this explanation is completely compatible with Dr. Levinson's dynamic vector theory of dyslexic symptom formation: inner-ear related dysfunction vs. compensatory mechanisms. In other words, all the many and varied dyslexic symptoms and their respective intensities are resultants of a dynamic combination of dysfunctioning inner-ear-related mechanisms on the one hand and compensating mechanisms attempting to minimize impairments on the other. Thus stress, anxiety, seasonal allergies, ear and sinus infections as well as any and all disorders impairing or destabilizing inner-ear functioning tend to maximize the intensity of symptom formation. By contrast, maturation, parental and educational support as well as favorable responses to a wide range of helpful therapies tend to minimize symptoms via compensatory functioning.
Needless to say, this clinically based and derived dynamic view of inner-ear determined dyslexic symptom formation with therapeutic and natural compensation clearly highlights the prior traditionalist fallacy of defining this highly fluctuating four dimensional disorder as if it were merely a simple two dimensional image fixed in stone. According to the mistaken traditional view, to be dyslexic, one had to be two or more years behind peers or potential in reading; being 1.9, 1.8, or 1.7 years behind wouldn’t count. And being severely behind in the typical non-reading dyslexic symptoms (i.e., writing, spelling, math, memory, speech, etc.) wouldn’t count, either.
Hopefully the following clinically-based and observed understanding of helpful methods will significantly contribute to every dedicated professional's ultimate aim: to find and use the best possible approach in order maximize the help that can be provided to all dyslexics, young and old. Dr. Levinson has little doubt that this ensuing holistic therapeutic force and synergy will inevitably lead to new and more effective therapeutic combinations.
Medical Treatment
The first and only medical treatment for dyslexia resulted from Dr. Levinson's discovery that this disorder was of inner-ear, or CVS, origin. Since the antimotion-sickness and related medications were known to improve the balance/coordination/rhythmic and related vertigo and motion-sickness symptoms characterizing inner-ear dysfunction, it seemed reasonable for Dr. Levinson to anticipate that these very same medications might be helpful for also improving many similar and related symptoms found characterizing the dyslexia syndrome. Fortunately for countless millions, this assumption was proven valid!
As the many and varied case presentations demonstrate on this website as well as in Dr. Levinson's many prior clinical studies and books, the inner-ear or CVS enhancing medications proved significantly helpful as chemical fine-tuners for all the sensory-motor and related memory, cognitive, ADD and anxiety/mood functions characterizing dyslexia. In addition, the combined use of nutrients and other chemical substances geared towards enhancing normal and abnormal CNS signal transmission and processing added synergistic potency to the overall treatment plan. As a result, medical treatment now offers more than 75–85% of treated dyslexics new hope and help while facilitating even greater favorable responses (~100%) to dyslexics provided with overlapping non-medical therapies.
Favorable Responses to Inner-Ear Enhancing Medications
Click to enlarge
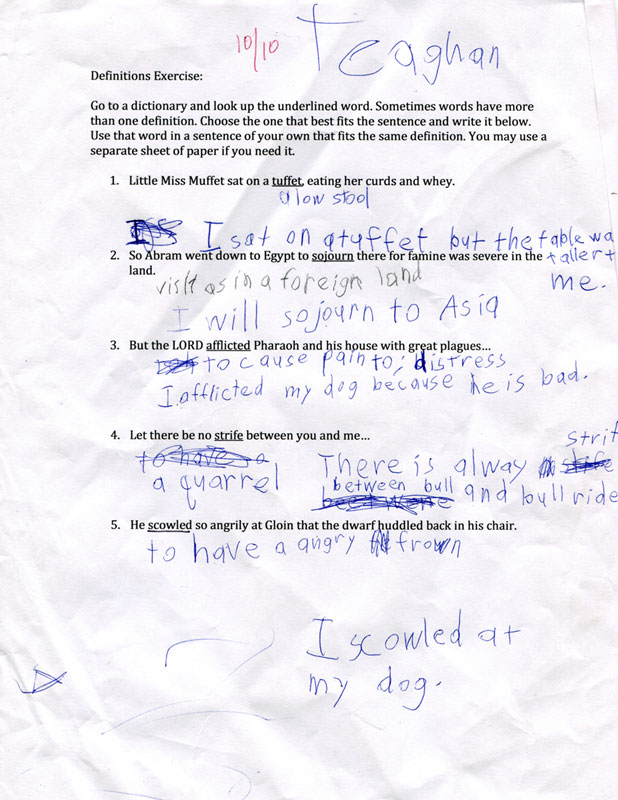
Patient Teaghan's handwriting prior to treatment.

Click to enlarge
Just one month after treatment, Teaghan's handwriting shows a dramatic improvement.

Luke is a very bright, determined but frustrated 10-year-old dyslexic. According to his mother:
"Almost instantly…he stopped tripping…dozing out and began telling us what happened each day. It's like he suddenly showed up for his life."

Teaghan was recently examined and treated for dyslexia. Although brilliant, his needed improvement was both rapid and dramatic.
Non-Medical Therapies
Nutritional/Allergic Treatment
In view of the fact that niacin, related B vitamins and minerals were many years ago reported to sometimes improve inner-ear-related dizzy and balance symptoms, the previously noted favorable findings of nutritionists in dyslexia became readily understandable — especially if we consider their possible compensatory role in enhancing both normal and abnormal signal transmission and processing. For example, ginger root was shown to be a highly effective antimotion sickness or inner-ear enhancing substance, so Dr Levinson used it for many, many years whenever needed. In addition, nutrients such as lecithin and ginkgo were shown to enhance memory while fatty acids and omega 3 can occasionally improve concentration. Also amino acids such as DL phenylalanine may decrease overactivity levels and increase focus in fortunate responders, thus occasionally avoiding the need for stimulants in a lucky few. These nutritional substances may also enable clinicians to decrease the dosages for needed stimulants and other medications, thereby reducing the risk of potential side-effects..
By contrast, Dr. Ben F. Feingold, a noted allergist, recognized that sugars, dyes, and various other allergenic substances may aggravate and even trigger such dyslexic/ADD-related symptoms as hyperactivity, impaired concentration and distractibility. Accordingly, the avoidance of these so-called “neurotoxic” substances in select individuals resulted in corresponding improvement. In Dr. Levinson's experience, allergies most often magnify or trigger pre-existing dyslexic/ADD symptoms by further destabilizing inner-ear-related functioning. They typically do not cause this disorder, unless the allergic attack is severe enough to primarily impair inner-ear and related CVS mechanisms and related brain structures.
Occupational/Sensory Integration, Reflex, & Optometric Treatment
Occupational/sensory integration, vestibular, and ocular therapists have reported academic and coordination improvements when dyslexics perform various motion-related and/or eye-training and sensory processing exercises. Inasmuch as the inner-ear or CVS controls all body and eye movements, it also controls all sensory and motion-related activities. Therefore, since repetition often leads to improvement in the specific sensory-motor task repeated, it seems reasonable to assume that practicing sensory-motor skills will result in an improvement in the inner-ear-related mechanisms governing them. However, one must still account for the reported academic improvements when only sensory and/or motor exercises are performed. In other words, why will a child given only eye and balance/coordination exercises read, write, and concentrate better? The answer is obvious if one goes back to Dr. Levinson's previously described concept of dyslexic mechanisms and functioning.
Transfer of Function: Specific vs. Generalized Improvement
Repetitive motor and selective reflex inhibition/enhancement tasks are known to improve underlying inner-ear and even higher brain interrelated mechanisms. If we assume that these specific improvements extend or are transferred to neighboring inner-ear-related circuits or channels, then we can readily explain the generalized improvements that often occur when specific sensory-motor "TV-like" channels or circuits are strengthened by repetition, practice, or conditioning.
For example, if repetitive eye-tracking techniques help fine-tune and stabilize its underlying "TV" circuit or channel e, and if this conditioned or improved effect is transferred to neighboring and interconnected circuits, i.e., channels r, w, m, c, t, etc., then reading, writing, math, concentration, and tennis will correspondingly improve. However, in many circumstances transfer of functional improvements to neighboring/interdependent circuits is restricted, thus accounting for the limitation characterizing the above therapies.
Perhaps a clinical illustration will be helpful in highlighting the above content. When astronauts and other experimental subjects were readied for space and spun in various directions, an interesting observation was noted: Rotating someone repeatedly in a counter-clockwise direction often led to an improvement in the tolerance for only counterclockwise rotations. Contrary to initial expectations, it did not invariably lead to improvement in tolerating clockwise and other types of directional rotations. This observation clearly indicates how the body specifically adapts to correspondingly specific stimuli and conditions, including changes in gravity, while resisting more generalized responses.
Athletics Improves Concentration and Cognition
Fortunately, the transfer of functional improvements to neighboring circuits does occur, at least in certain contexts. In his clinical experience, Dr. Levinson has repeatedly noted the existence of an initially puzzling and strange phenomenon: Dyslexic athletes often do best academically when in training, despite the limited study time they have. Upon termination of their sports activities, due to either a changing season or an injury, or even punishment for prior academic failures, a significant number of athletes report a corresponding decrease in their concentration, memory, and overall academic functioning.
At first glance, one might mistake this correlation as an excuse conjured up by athletes to justify their training time. This was not the case, however. Most often it was their parents who reported this fascinating but puzzling correlation. It therefore appeared that sports activities and exercises resulted in a transfer of function to neighboring/interconnected and/or underlying inner-ear-related circuits, which in turn resulted in academic/concentration improvements. Unfortunately, cessation of practice often led to a regression in underlying functioning, and the conditioned transfer of function was in turn eliminated. The unexpected clinical observation that physical exercises in dyslexics may result in increased mental capacity is in accord with the adages "Practice makes perfect." and "Sound body, sound mind." And it is in perfect harmony with the sensory-motor therapies developed by Ayres, Belgau and both Peter and Sally Blythe.
Moreover, these observations help explain why there are so many seemingly “crazy joggers” running miles and miles in the early morning prior to work. Obviously, they wouldn’t do it if they didn’t feel better. Indeed, jogging and a variety of other exercises must clearly fine-tune their CV and related brain systems and thus force enhancement of their overall daily functioning.
Yoga and the Inner-ear Connection
The growing popularity of the practice and beneficial therapeutic results of yoga have thus far defied a proper neurophysiological explanation. After meeting with Ila and Garrett Sarley as well as Stephen Cope at Kripalu and reading their brilliant works, it became clear that the movement/timing/concentration/enhancement provided by yoga is also CVS modulated — a concept requiring further study. Is it any wonder that millions of individuals practicing yoga report significant improvements in balance/coordination/rhythm, concentration, cognition, decreased anxiety and stress as well as corresponding feelings of well being and contentedness? Even being in greater touch with or harmony with our body, mind and surroundings has a crucial CVS component!
Chiropractic & Dental Treatment
Patients have occasionally reported to me symptomatic improvements arising from chiropractic manipulation and/or dental corrections of their temporomandibular joint (TMJ). Needless to say, these observations are as valid as any other type and must be accounted for rather than "criticized" away. It is well known that many dyslexics will tilt their head, neck, and body in order to read, write, and concentrate better. The neck is an important integration point for the inner-ear-related circuitry. Perhaps the chiropractic adjustment of these and other body positions serves a similar purpose to that performed instinctively and reflexively by dyslexics from within — by tilting their heads and finding varied body positions more favorable for reading, concentration, etc.
Dental problems and procedures affecting the temporomandibular joint may often lead to headaches, dizziness, impaired concentration, and dyslexia-like functioning. To explain these inner-ear-related symptoms, Dr. Levinson reasoned that an inflammation or misalignment of the temporomandibular joint may indirectly affect the neighboring inner-ear systems, thus either mimicking or aggravating dyslexic symptoms. Accordingly, proper dental intervention may result in a corresponding improvement.
Educational Therapies — Special and Otherwise
Educational therapy is as complex as it is crucial. And since each dyslexic child or adult is uniquely defined by their normal vs. abnormal pattern of specific perceptual memory, concentration/distractibility and related cognitive functions it is imperative that educators attempt to understand their students’ assets and deficiencies before applying compensatory techniques.
Needless to say, this rather daunting task is easier said than done. It requires that educators be armed with a vast array of compensatory educational techniques admixed with gifted intuitive and empathic functioning as well as the crucial neurophysiological insights provided within this and related works. In the final analysis, teachers are expected to perform Herculean “wonders” on large groups of desperate children and adults, often without the help and guidance of clinically experienced experts.
In general, it appears logical for educators to impart vital information by finding and utilizing clear and relatively open (non-scrambled) channels while also attempting to improve minimally impaired functions and channels via repetition and other techniques. Thus there is value in attempting a multi-sensory-motor approach initially — until more specific insights are obtained through repetition and trial and error.
Visual & Auditory Therapies — Special & General
The adage “practice makes perfect” has therapeutic value not only for dyscoordinated motor tasks but for scrambled sensory and secondarily related cognitive functioning as well. Just as repetitive motor tasks often lead to improvements in both the specific underlying determining mechanisms and to neighboring, overlapping or interdependent circuits via a more generalized functional transfer, the same holds for repetitive visual, auditory and related sensory therapies.
These rather “simple” neurophysiological insights utilized by both occupational or sensory-motor therapists as well as educators also help explain the efficacy of both visual and auditory training, albeit the latter often utilizes patterns of non-cognitive stimuli. In other words, if a given sensory input drifts, the corresponding messages to the thinking brain are blurred, reversed, or scrambled, making it difficult to remember and/or understand. Moreover, these drifting or blurred imprints are frequently wiped-out or rapidly erased because they are perceived as faulty. Sensory repetition and conditioning therapies frequently force compensatory brain changes and adaptations in which these drifting visual and auditory inputs are finally descrambled and “imprinted” or accepted for storage and memory retention. In other words, the underlying inner-ear-related and other mechanisms are triggered to compensate and even overcompensate in a manner similar to the way repetitive motor (and educational) tasks force both an improvement in the balance and coordination circuits as well as an enhancement of the compensatory processing abilities of other vital normal brain mechanisms and structures.
Tinted & Magnification Lenses
The use of tinted lenses was recognized to be helpful in minimizing or compensating for the various reading symptoms characterizing dyslexia. Since inner-ear dysfunctioning subjects may be light-sensitive or photophobic due to impaired light-wave or glare filtering, it appears reasonable that tinted lenses may be as helpful for some dyslexics as is increasing the print size in reading material for others. In addition, both color and increased target size enable the eye as an inner-ear-directed guided missile to better concentrate on and hit its target. Thus, one or both of these mechanisms can readily explain the benefits provided by this therapy.
Psychotherapy
Psychoanalysts, psychiatrists, and related professionals previously believed child-rearing and emotional disturbances were primarily responsible for many learning, concentration, emotional, mood, anxiety and behavioral symptoms that characterized inner-ear dysfunctioning dyslexics. Consequently, a host of very specific psychologically-based subtheories and mechanisms were mistakenly formulated in order to account for each of the many dyslexic-related symptoms. Invariably, psychotherapy was ill-advised in an effort to cure or alleviate the emotional factors erroneously deemed primarily responsible for these symptoms.
The fact that psychotherapy may alleviate a dyslexic's symptoms does not prove that psychological factors caused the core disturbance. Indeed, psychotherapy often alleviates stress and secondary feelings of stupidity, frustration, and helplessness. However, these are factors that secondarily complicate and destabilize an already impaired fine-tuning system. In other words, the surface psychological and behavioral symptoms resulting from a primary inner-ear impairment are often important secondary reactions to the dyslexic's inability to function and compete normally. And as a result, medical and psychological treatment may often be required to attain maximum overall improvement.
The Therapeutic Value of Insight ➤Biofeedback & Cerebral-Enhancing Therapies
The cerebral cortex and the "higher cerebellum" were found by Dr. Levinson to play a major compensatory role in dyslexia. As a result, biofeedback and any related conditioning or learning therapy that stimulates and enhances thinking brain functions may significantly improve dyslexia and it's underlying CV dysfunctioning.
The Neurological Approach
The traditionalist neurological approach to dyslexia was significantly guided by the mistaken belief that this disorder was due to a primary rather than a secondary dysfunction within the thinking-brain, the seat of our intellect and language functioning. Since no medical therapy to date can "cure" an impaired thinking-brain, the neurological method of treatment consisted of referrals to educators for Special Ed.
In retrospect, both psychiatrists and neurologists were similarly misled. They mistakenly believed the secondary fallout of the dyslexic disorder to be its primary cause. Neither specialty was capable of finding a primary cerebral therapy that worked because it did not exist.
Summary
A series of varied medical and non-medical dyslexia therapies have been presented and discussed. When these and other non-reviewed therapies are properly understood and utilized via a holistic approach, all dyslexics can be helped and all possible favorable responses will be maximized.
By contrast, the traditionalist theories have led nowhere medically. Were these theorists able to have taken "only one step for man" by listening to Huxley's simplistically brilliant research dictum "to give up every preconceived notion" and to "follow humbly wherever and to whatever abyss nature leads," there would by now have resulted "one giant leap for mankind." But sad to say, the traditionalists failed to heed Huxley’s commonsense but ingenious advice, just as they failed to listen to their dyslexic patients. They remain opposed to all ideas except the mistaken alexia/dyslexia theoretical constructs and equations. However, the recent validation of the cerebellar role in dyslexia suggests that the century-old opposition to groundbreaking insights and treatment are fading — and hopefully may even soon disappear.
THE THERAPEUTIC VALUE OF INSIGHT ➤Yoga

Enhancing cognition and concentration
Sensory-Motor Integration

Motion improves inner-ear functioning
Exercise

Improving Dyslexia and ADD
Nutrients

Enhancing brain activity
Play Therapy

Enhancing self-esteem
Reflex Therapy
Triggering sensory-motor development
Insight / Self-Esteem Therapy
Psychotherapeutic Insight

Neurotherapeutic Insight
Enhancing psychological and neurological insights improves self-esteem. Learn more about Insight Therapy ➤